The Hidden Cost of Physician Burnout and Turnover
Physician burnout and turnover represent one of the largest untracked cost centers in healthcare systems today. Replacing a single physician costs between $500,000 and $1.2 million depending on specialty — before accounting for the downstream effects on patient experience, team culture, remaining physician workload, and organizational risk.
What makes this cost uniquely difficult to manage is that the departure is rarely sudden. Physicians disengage long before they resign — and during that invisible window, performance metrics can remain stable while the system quietly accumulates cost it won't see for months or years.
The Pattern Most Systems Are Already Experiencing
This is not a new problem. Healthcare executives have been watching physician attrition for years, investing in wellness programs, leadership initiatives, and engagement surveys — and watching the exits continue anyway.
The reason those investments have underperformed is not a budget problem or a leadership failure. It is a measurement problem. The metrics most systems use to track physician health — engagement scores, survey participation, productivity numbers — measure output and compliance. They do not measure the variable underneath: whether the work is still giving something back to the physicians delivering it.
By the time the data moves, the decision to leave is already forming. Sometimes it has already been made.
"The system is extracting efficiency faster than it is replenishing meaning — and that imbalance shows up as cost."
That is the hidden cost of physician burnout. Not the exit itself — but everything that happens in the long period between disengagement and departure, while dashboards still look strong.
What This Actually Looks Like From the Inside
Dr. Gigi Abdel-Samed spent more than 30 years as an emergency physician. By every external measure, she was succeeding. Associate Medical Director of a Level 1 Trauma Center by 32. Medical Director of a community hospital ER at 36. Associate clinical professor. Multiple board certifications. A lake house. A city home.
And she was quietly disappearing.
The erosion didn't announce itself. It accumulated — in the gap between what medicine demanded and what it returned. She kept performing. The metrics looked fine. And underneath that performance, she was losing her connection to the reason she had become a physician in the first place.
It progressed into addiction. Into a period where she had to step back from medicine entirely — not because she had stopped caring, but because she had been running on depletion for so long that the system holding her together finally gave way.
What she found on the other side of that was not a different career. It was the same medicine — restored. The work hadn't changed. What changed was her relationship to it. She separated her identity from her title. She reconnected to the original reason she had walked into an emergency department at all.
"For a long time, medicine wasn't just my career — it was my identity. And when something becomes your identity, every hard shift feels personal. Every mistake feels defining. Every doubt feels like a verdict."
That insight — that the problem is not medicine itself but the erosion of meaning inside it — is what Medical School for the Soul is built on.
And it is not unique to Dr. Gigi. It is the pattern she has watched repeat across 30 years of clinical practice, and the pattern she now helps healthcare systems interrupt before it becomes a cost event.
What Disengagement Looks Like in a High Performer
Dr. Frank is a senior physician — accomplished, respected, the kind of clinician other physicians trust without question. When he began the work with Dr. Gigi, nothing in his professional presentation suggested a problem. His performance was strong. His patient relationships were intact.
What emerged quickly was something that has nothing to do with clinical competency. Patterns from childhood — the roles he had learned to play, the ways he had learned to absorb pressure and keep moving — had become the invisible operating system running his professional life. He had never connected them to what he was experiencing at work. Nobody had asked him to.
He took up painting. Not as a hobby — as an intervention. It connected him to something from his early life, to relationships and memories that pre-dated medicine entirely. That reconnection created a channel back to himself that his clinical identity had closed off.
His performance did not change. What changed was what the performance cost him. The work started giving something back.
That is what disengagement looks like in a high performer. Not a decline in output. A quiet exhaustion of the person producing it — invisible to every dashboard, visible only to the physician living it.
The Costs That Don't Have a Line Item
When physicians disengage before departing, systems absorb cost across four areas simultaneously — usually without connecting them to a single upstream cause.
1. Patient Experience
Physician presence is the primary driver of how patients experience care. When presence erodes — when a physician is technically competent but internally depleted — encounters feel transactional. Patients report feeling rushed, unheard, unseen. HCAHPS scores plateau despite operational improvements. Complaints accumulate. Trust weakens slowly, then noticeably.
This is not a communication training problem. It is a presence problem. And presence cannot be trained into a physician who has lost connection to why the encounter matters.
2. Retention and Replacement
The financial cost of losing a physician is well-documented. What is less discussed is the timeline. Physicians typically disengage 12 to 24 months before they resign. During that window, they are absorbing a full salary and benefits package while delivering care at a fraction of their previous engagement level — and the system has no mechanism to detect it.
When the resignation comes, it often feels sudden to leadership. It was not sudden. It was cumulative.
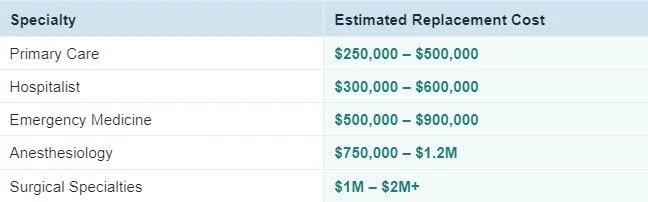
Sources: MGMA, NEJM Catalyst, Merritt Hawkins. Figures include recruiting, signing bonuses, onboarding, ramp-up time, and lost patient revenue. Conservative estimates used throughout.
3. Risk Exposure
Cognitive overload, emotional depletion, and reduced presence are documented contributors to medical error and adverse events. Physicians operating at the edge of their capacity — compensating for system friction, absorbing patient frustration, making high-stakes decisions under time pressure — carry a risk profile that does not show up in credentialing files or performance reviews.
By the time risk materializes in a complaint or litigation event, the underlying cause has been building for months or years. MSFTS operates upstream of that timeline.
4. Cultural Degradation
Disengaged physicians do not simply leave. Before they leave, they stop mentoring. They stop advocating. They stop bringing discretionary effort to team dynamics, leadership initiatives, and organizational culture. The physicians around them notice. The pattern spreads — quietly, without triggering any alert.
Culture does not erode in a single event. It thins over time, through a hundred small withdrawals that never register individually.
Why Current Solutions Don't Interrupt This Pattern
Most physician support programs share a structural design flaw that limits their effectiveness regardless of their quality or intent.
They operate outside the workday. Wellness apps, resilience workshops, EAP resources, off-site retreats — all of these address physician experience after the clinical encounter. But the erosion happens inside the encounter. In the compressed moments between patients. In the gap between what medicine demands and what it returns.
You cannot restore presence by intervening after it is depleted. You cannot rebuild meaning by offering support at a time when the physician has already left the context where meaning lives.
The second structural flaw is framing. Most programs — even good ones — position the physician as the problem to be solved. They ask physicians to cope better, manage stress more effectively, build resilience. High performers reject this framing instantly. It reads as: the system is fine, you need to adjust. That message does not earn trust. It accelerates cynicism.
The result is a pattern most systems recognize: programs are funded, utilization is low, physicians remain skeptical, and the exits continue.
"We don't need more support programs. We need a way to protect the human variable our performance depends on — in real time."
What Actually Stops the Pattern
Interrupting physician disengagement before it becomes a cost event requires operating where the erosion actually happens — inside the workday, inside the encounters, inside the moments where meaning is either present or absent.
Medical School for the Soul was designed for exactly that layer. It does not ask physicians to add time, attend meetings, or process their experience publicly. It works through the Refined Source Code Method™ — a framework that helps physicians identify and interrupt the operating patterns driving invisible exhaustion, and reconnect to what brought them into medicine before the system had fully extracted it.
The result is not a physician who feels better about a bad situation. It is a physician for whom the same clinical encounter costs less — and returns more. That shift is felt first in presence, then in patient experience, then in retention.
→ See how it works in your organization
NEXT STEP FOR HEALTHCARE LEADERS:
If you’re evaluating physician retention, engagement, or culture within your organization:
→ Request an executive briefing
Frequently Asked Questions
What does it cost to replace a physician?
Replacing a physician costs between $250,000 and $2 million or more depending on specialty, when accounting for recruiting fees, signing bonuses, onboarding, ramp-up time, and lost patient revenue. Emergency medicine averages $500,000–$900,000. Surgical subspecialties often exceed $1 million.
How does physician burnout affect patient outcomes?
Physician depletion reduces presence during patient encounters — patients report feeling rushed and unheard even when clinical care is competent. This drives flat or declining HCAHPS scores, increased complaints, and eroded patient trust independent of clinical quality.
Why do wellness programs often fail to solve physician burnout?
Most wellness programs operate outside the workday, where they cannot reach the moments where meaning erodes. They also inadvertently frame physicians as the problem to fix — a framing high performers reject. Low trust and low utilization are the predictable result.
What is the financial impact of physician disengagement before resignation?
Physicians typically disengage 12–24 months before they resign. During that window, systems pay full compensation while receiving reduced engagement, presence, and discretionary effort — without any dashboard signal that the cost is accumulating.
How does burnout affect hospital culture?
Disengaged physicians stop mentoring, stop advocating, and withdraw from organizational initiatives before they formally leave. This withdrawal spreads — other physicians notice, cynicism increases, and culture thins without triggering a measurable alert.
What is the difference between physician burnout and physician disengagement?
Burnout refers to the clinical syndrome of exhaustion, depersonalization, and reduced efficacy. Disengagement is the earlier, operationally more significant stage — when a physician is still performing but meaning has eroded and return-on-effort has collapsed. Disengagement precedes burnout and is far more costly because it is invisible longer.
How early can hospitals detect disengagement before it becomes expensive?
Standard tools — surveys, productivity metrics, engagement scores — detect disengagement late, after the decision to leave is often already forming. The most effective intervention is upstream: stabilizing the human variable before the cascade begins, rather than measuring it after it advances.
Have more questions? Visit the full Physician Burnout & Retention FAQ.